PACU Neuraxial and Regional Guidelines
![]() Click on Graphic to download PACU Neuraxial and Regional Guidelines file (130 KB)
Click on Graphic to download PACU Neuraxial and Regional Guidelines file (130 KB)
EPIC ORDER SETS TO USE:
- Multimodals + catheters: IP PAI Peripheral Nerve Catheter/Regional Analgesia Admit
- Epidural orders (need to still use above order set for multimodals): IP PAI Epidural Analgesia Postop
ORTHO: Manage catheters and multimodals
- Ensure home meds restarted (if questions, d/w pain fellow/attending/APP for CURES report). Primary team should write for
- FOOT/ANKLE: NO Celebrex
- SHOULDER/ARM: gabapentin ok, NO Celebrex/nsaids
- CHEUNG/COSTOUROS/CHOU: write for catheter, oxy 5-10mg q3hr prn, adjuvents ok, no Celebrex
- If you need to bolus for pain an ISC/supraclavicular/infraclavicular in PACU, please start first with only 3-5cc ¼%bupi or 0.2%ropi or check with regional
- SPINE: ALAMIN-surgical epiduralàwrite epidural cath orders (d/w alamin each case if wants only local anesthetic or +/- epidural opioid), ok to write for multimodals in epidural pts, no gabapentin unless home med
- TRAUMA: d/w trauma if ok to write for nerve block infusion when patient comes out (or if they need neuro exam first once wake up from anesthesia), can write multimodals in catheter pts
- Amantullah hips (if catheter): ok for oxy prn, gabapentin, Tylenol atc, Celebrex ok if pt appropriate for
- MULTIMODAL MEDS:
- Oxycodone 5-10mg q3hr prn (adjust dose for age and baseline chronic pain meds as see fit, ie example 2.5-5mg for older age or if chronic opioid use, expand range 5-15mg )
- Tylenol 650 q6hr
- Gabapentin 300mg TID (unless >70yo, then 100mg TID vs 100mg qHS vs none)
- All nerve catheters (with exceptions listed below for TAP, QL, ESP, PVB, epidurals)
- Ropivicaine 0.2% continuous 5ml/hr + 5ml q30min
- If 2 nerve catheters (ie pop/saph), write 0.1% ropi continuous 5ml/hr +5ml q30
- Quadratus Lumborum (QL)/Transversus abdominis plane (TAP) (other than plastics)
- Single catheter: 0.2% ropi autobolus 10mlq 60min + 5ml q 30min pt demand
- 2 catheters: 0.1% ropi autobolus 10ml q60min +5ml q30min pt demand
- Paravertebral (PVB)
- Single catheter: 0.2% ropi autobolus 10ml q 60min + 5ml q 30min pt demand
- 2 catheters: 0.1% ropi autobolus 10ml q60min +5ml q30min pt demand
- Erector spinae plane (ESP)àWhat should the orders be for this, especially when bilateral??
- Single catheter: 0.2% ropi autobolus 10ml q 60min + 5ml q 30min pt demand
- 2 catheters: ???to be decided at regional conf 2/9 and updated
- PLASTICS AND RECONSTRUCTIVE SURGERY: TRAM flaps. Plastics primary to write multimodal pain meds
- TAP catheters (2 catheters): 0.1% ropi autobolus 10ml q60min +5ml q30min pt demand.
- STUDY catheters: do NOT bolus in PACU. Plastics team to order nerve block meds and all pain orders, Look for pt status as “study patient” in daily regional email and write that on acute pain handoff summary line ***STUDY PATIENT***
- THORACIC EPIDURALS: manage epidurals ONLY. Multimodals per primary thoracic team
- Shrager: no opioids in epidural
- Berry/Backhus: epidural ok with bupi/HM/fent PCEA
- UROLOGY: when an epidural in place, manage epidurals, ok for bupi/HM/fent PCEA.
- Dr. Gill Harcharan: ok for pain team to write for multimodals as above + epidural orders
- EPIDURALS
- Bupi 1/8th% @6ml/hr
- Dilaudid: age <55yo: 0.2mg/hr, 55-65yo: 0.1mg/hr, >65yo: 0.05mg/hr
- Fentanyl PCEA 10-25mcg q 10min
- SPINALS
- If duramorph given in spinal, add to pain list for pain service to do post-op check in AM
- CARDIAC SURGERY: primary service to write multimodals
- PVB vs ESP: see above nerve pump orders
LIDOCAINE DRIP
- If you think a patient needs a lidocaine gtt on the floor or to continue on floor from intraop, must have primary surgical team page acute pain pager 27246 to formally consult and given signout. Ok for pacu resident to start lido gtt in PACU.
- To Order, open up an order set and scroll to the bottom to “Ad-hoc orders” and search for lidocaine. In the pop-up window, click on facility list tab and select under panel order set: lidocaine infusion and consult panel (PAIN) to order. If obese patient, make sure to order 1mg/kg/hr at IBW or LBW (and not TBW, otherwise get toxicity faster/higher lido levels)

GENERAL FLOW FOR ACUTE PAIN PATIENTS:
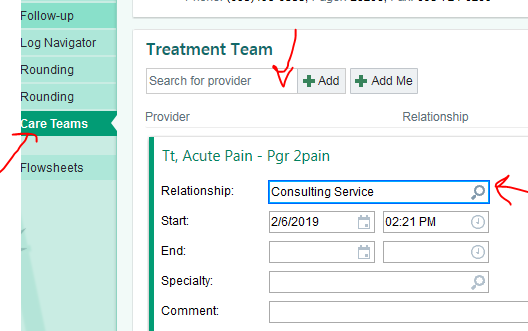
- Add patient to acute pain list: Care teamsàenter “tt acute pain” in treatment teamàselect “consulting service” for relationship
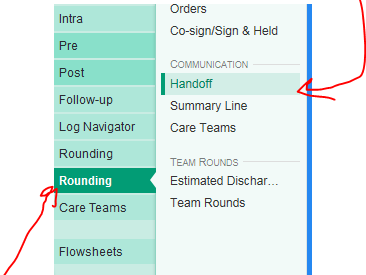
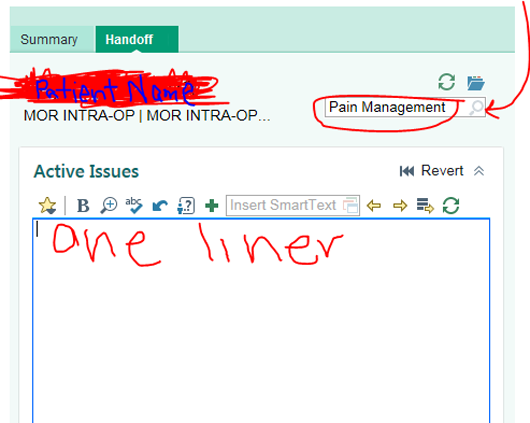
- Write handoff summary line: Rounding tab in navigatorà”handoff”àunder magnifying glass in window that pops up on right side, select “pain management”àwrite one liner and orders written for
- Place orders per above guidelines

